All Categories
All Categories
I was standing next to a client between sets while he sat on the edge of the bench, phone in hand. He turned the screen toward me and asked what his recovery score meant for the rest of the session.
He had not slept well, his HRV had dropped, and his wearable told him he was not ready to train hard. He did not ask whether he should lose fat or get stronger. What he asked was whether the numbers meant something was wrong. If you coach adults now, the longevity conversation is already in your room. That is why the longevity coaching panel at Career Lab matters.
Career Lab by Coach360 comes to Las Vegas on July 17 and 18, 2026, built around a simple promise: build the career you want in fitness, and grow it, expand your business, and earn CECs in a single day designed for your growth. It is not a sit-and-listen conference. The day blends strategy, community, and movement, so you leave having actually built something.
The format is hands-on. Focused breakout sessions put you in small groups where you can ask questions and get tailored guidance across brand, business, and coaching tracks. Workshops have you working on your offers, pricing, content, and career strategy with live support. A Move & Mingle group workout connects you with other fitness pros through training rather than small talk. The agenda runs from a morning keynote on designing your 2026 career roadmap, through breakouts and an afternoon keynote, into the industry-leader panel block in the early afternoon, and closes with a session that turns the day into a concrete 2026 plan. You also earn CECs recognized by major certification bodies, which is part of why coaches treat the day as professional development rather than a networking detour.
The longevity panel sits inside that block of real talk with industry leaders. It is built for the coach who keeps getting the recovery-score question on the gym floor and wants a sharper answer than a shrug. The panel is set to focus on recovery, biomarkers, sleep, performance, and long-term health strategy, with industry leaders and familiar faces including Dr. Jonathan Mike, Faithlyn Derla, Bob Thomas, and moderator Nathan Hyland.
“This event brings together people who are serious about growing, evolving, and redefining what success in fitness really looks like, and that’s a conversation worth being in.”
— Dr. Jonathan Mike, Owner of Scientific Strength
Coaches are no longer only managing workouts. They are managing client expectations around healthspan, recovery, readiness, and wearable data. The panel exists because that shift is already here, and the coaches who handle it well are the ones with a method, not an opinion.
ACSM named wearable technology the No. 1 global fitness trend for 2026, and noted that nearly half of U.S. adults now own a fitness tracker or smartwatch. Clients now walk into sessions with numbers before they have any context for them. Before you explain a wearable score, ask what changed first: sleep, stress, soreness, travel, food, alcohol, illness, or training load.
The goal is to slow the conversation down before a single metric becomes the whole plan, not to turn the coach into a clinician. A coach can use data to ask better questions. They can adjust load, shift intensity, track patterns, and discuss habits. What they should not do is diagnose a lab value or turn a wearable score into a medical conclusion.

Poor sleep, high soreness, and low readiness should change how you coach the day. They should not push you into diagnosis. The American Heart Association includes sleep in Life’s Essential 8, alongside physical activity, diet, nicotine exposure, weight, cholesterol, blood sugar, and blood pressure. The AHA sleep metric recommends 7 to 9 hours of sleep daily for optimal cardiovascular health in adults, and the CDC places physical activity inside chronic disease prevention, where 150 minutes of moderate weekly activity can reduce disease risk.
A client with poor sleep, heavy soreness, high stress, and weak readiness does not need blind intensity. They need a coach who can read the week and adjust the session: holding load, moving from intervals to Zone 2, reducing volume, or changing the day’s goal.
“I love seeing these coaches show up hungry to receive from all the speakers and panelists. And best yet, we all learn from each other.”
— Nathan Hyland, Co-Founder & Managing Partner, Lapaix Hyland GBC
Life’s Essential 8 includes blood pressure, cholesterol, blood sugar, and weight, and notes that hemoglobin A1c can reflect long-term blood sugar control in diabetes or prediabetes. That still does not make lab interpretation a coaching job. An evidence-based longevity coach should ask whether a clinician reviewed the result, ask what guidance the client received, and align exercise habits with that guidance. They should not diagnose, prescribe, adjust medication, or explain abnormal labs.
Use this cue:
“Bring that result back to your clinician. Once they give you guidance, I can help you build the habits around it.”
That line protects the client as well as the coach. The coach’s job is to support training, recovery, movement, and behavior inside scope. It is the clinician who should be in charge of interpreting the marker.
Longevity-advantage clients are asking for more than hard sessions. They want:
ACE’s 2025 healthspan guidance gives practical strategies for health coaches and exercise professionals, built on aerobic training, resistance training, balance, flexibility, structured sessions, and lifestyle activity. A coach who understands longevity builds repeatable systems around strength, aerobic work, mobility, recovery, sleep habits, and consistency.
Use this as the referral framework for longevity coaching.
Clients need coaches who can help them train better. They also need coaches who know when the answer belongs to a clinician.
More data can improve coaching, but it can also create noise. Wearables can drive anxiety, and biomarker talk can drift into medical advice. One bad sleep score can make a coach overcorrect, and one readiness score can distract from the bigger pattern. Your job is not to chase every metric. It is to notice patterns, adjust training, and refer when the signal belongs outside coaching. That is the kind of discipline longevity coaching requires.
Related: Longevity Fitness Coaching: How to Shift Clients From Short Cuts to Long Games
The Longevity Advantage panel takes place at Career Lab Las Vegas on July 17. Coaches will hear how leaders are thinking about recovery, sleep, biomarkers, performance, and long-term client health strategy, and will leave with CECs and a 2026 plan.
Reserve your seat at coach360news.com/career-lab-by-coach360-vegas
What is the Longevity Advantage panel at Career Lab?
It is a Career Lab Las Vegas panel on what clients expect from coaches around recovery, sleep, biomarkers, performance, and long-term health strategy. It sits inside the event’s industry-leader panel block and is built for coaches who are already fielding wearable and readiness questions on the floor.
What should an evidence-based longevity coach know?
An evidence-based longevity coach should understand strength, aerobic training, recovery, sleep, habit design, biomarker awareness, and referral boundaries. They support health behaviors without diagnosing or treating, and they know which questions belong with a clinician.
Can coaches talk about biomarkers with clients?
Yes. Coaches can ask whether a clinician reviewed the result and can use provider guidance to shape training support. They should not interpret labs, diagnose, prescribe, or adjust medication. The line is between supporting the habits around a result and interpreting the result itself.
Why does sleep matter in longevity coaching?
Sleep affects recovery, readiness, energy, and training response. Coaches can support basic sleep habits and adjust programming around poor recovery. They should refer when signs point to a medical sleep issue, such as a suspected sleep disorder.
This article previews a Career Lab by Coach360 panel and is intended as professional education for fitness coaches. It does not constitute medical advice. Interpreting labs and biomarkers, and any decisions about medication or treatment, belong with a qualified clinician.
I had a client who had tried continuous glucose monitoring (CGM) for two weeks. She wanted to know what it meant for her programming and her performance. I had seen maybe four CGM readouts prior to hers. I told her the truth: I could see patterns, but I was not the right person to tell her what the numbers meant medically. What I could do was tell her what the patterns suggested about when her body was ready to work hard.
That is the actual scope of what CGM data can do for a working fitness coach. Not more than that. And for a surprising number of clients, it turns out to be enough. If you are seeing CGM data show up in client conversations more often, you are not imagining it. Consumer-grade continuous glucose monitors have become widely available in the last two years, and a subset of fitness-forward clients are wearing them before they have any metabolic diagnosis. Some of that data is genuinely useful. Some of it is noise. And much of it is outside your scope regardless of how clearly the pattern shows up on the trace.
The skeptical-but-fair take on CGM for coaches is this: the technology produces a real signal. The error is in assuming the signal is more specific than it is, or that it belongs in a coaching conversation the same way it belongs in a clinical one. Those are two different conversations. The coaches who handle CGM data well are the ones who know, in the moment, which one they are sitting in.
Coaches who get their hands on CGM data for the first time do the same thing: they find the glucose number and try to figure out what it means. That instinct is understandable. A fasting glucose of 98 mg/dL means something when a physician is reading it alongside two years of labs, a medication list, and a clinical history. Sitting across from you in a gym, with none of that context, it means almost nothing you can act on. What you can act on is movement. How the trace shifts across a week of training days. Whether it drops when the client said they fell apart in the back half of a session. Whether the overnight pattern looks different on days when recovery feels off. That is the signal worth reading.
The data is a behavioral mirror, not a diagnostic tool. It shows you the relationship between what a client does and how their physiology responds. That is genuinely useful coaching information. But it is easy to overclaim, and overclaiming with health data in a fitness coaching context is both a scope-of-practice issue and a trust issue. Clients who bring you CGM data are often already in a slightly anxious relationship with their own numbers. The coach who meets that data with overcalibrated confidence is not helping.
“The usefulness of a CGM (or any biometric monitor), is in viewing the data through the lens of the client’s experience. Too often, clients want the data to generate some type of discrete value judgment about the quality of their performance. This externalizing undercuts the real value of monitoring, which is to put numbers to what the client is already feeling and experiencing and to present opportunities for behavior change.”
— Jonathan Ross, Creator of Funtensity, Two-Time Personal Trainer of the Year Winner, Author, Alzheimer’s Fitness Specialist Course
Four things are worth knowing about what a CGM trace actually shows on a training day, what it does not show, and where your read adds value. Those four things are what the rest of this piece is built around.
The trace shows glucose availability in real time. On a training day, you will typically see one of three patterns. A gradual decline during moderate-intensity work as muscle tissue draws on circulating glucose for fuel. A spike-then-drop during high-intensity intervals as the body releases stored glucose through glycogenolysis faster than it is being cleared. Or a relatively flat line during low-intensity zone 2 work, where fat oxidation is doing more of the fueling and glucose demand is lower.
Each of those patterns is normal. None of them is a problem on its own. What makes them useful is comparing them to how the client felt and performed during that session. A client who shows a sharp post-interval drop and reported feeling terrible in the back half of that session has a data point worth noting. “Your trace shows a significant drop right around the time you said you hit the wall. That pattern is worth watching across a few more sessions before we draw any conclusions” is a coaching observation. It is not a diagnosis. It is a reason to keep looking.
Where coaches get in trouble is in treating a single session’s trace as explanatory. One day’s glucose data is anecdote. Two weeks of training-day overlays, cross-referenced with the client’s self-reported energy and performance, starts to look like a pattern. The honest tradeoff in working with CGM data is that the meaningful signal takes longer to accumulate than most clients expect when they show up excited about their new sensor. Managing that expectation is part of the job.
CGM data does not tell you why the pattern is happening. A pre-session glucose of 72 mg/dL might mean the client undertimed their pre-workout meal. It might mean they are in a caloric deficit. It might mean they slept four hours. It might mean something their physician needs to evaluate. You cannot tell from the trace alone, and guessing out loud is worse than saying nothing.
It does not tell you what the client’s target range should be. Consumer CGM platforms display reference ranges, but those ranges are calibrated against population averages that were largely derived from clinical studies of people with metabolic conditions. A non-diabetic client wearing a CGM for performance awareness is not the population those reference ranges were designed for. Research in exercise physiology and metabolic health has documented that healthy, well-trained individuals can show glucose excursions during high-intensity exercise that would flag as abnormal on a standard clinical reference range, and that those excursions are physiologically unremarkable in a fit, non-insulin-resistant person. Telling a client their glucose “spiked too high” during sprint intervals, without that context, is a way to create anxiety that the data does not support.
It does not replace subjective self-report. This is the one coaches are most likely to underweight when the data is in front of them. A client who says they felt strong during a session where the glucose trace looks messy is giving you more useful programming information than the trace alone. The trace is context. The client’s experience is the primary data.
“The trace is context. The client’s experience is the primary data.”
And it does not, under any circumstances, belong in a conversation about medication, supplementation to manage glucose levels, or dietary changes designed to alter the trace. Those conversations belong with a physician or a registered dietitian. If a client asks you whether they should try berberine because they read it helps with glucose, the answer is: “That is a question for your doctor, not for me. What I can do is make sure the training side of this is working well for you.” Say it clearly and without apology. The clarity protects the client and it protects you.
The workflow below is built for coaches who are working with clients who already have CGM data or who are about to start wearing a sensor. It is not a protocol for recommending CGM to clients who have not asked about it. That recommendation crosses into clinical advice territory that coaching scope does not cover. If a client asks whether they should try a CGM, a reasonable answer is: “It can produce useful training information. I would run it by your doctor first, especially if you have any history of metabolic concerns.” That is the extent of the recommendation. For clients who are already wearing a sensor and want to integrate the data into their training, the four steps below create a structure that keeps the coaching work inside scope while making genuine use of the signal the data produces.
| Step | When | What the Coach Does | What to Avoid |
|---|---|---|---|
| 1. Baseline Read | Weeks 1–2 of the block | Ask client to share 7–10 days of CGM trace before any programming decisions. Look for fasting baseline, post-meal spikes, and overnight pattern only. | Do not interpret specific glucose values as diagnostic. Do not suggest targets. Note patterns only. |
| 2. Training Day Overlay | Weeks 3–4 | Ask client to log session start time, duration, and subjective energy rating (1–10) alongside the CGM trace for two weeks of training days. | Do not use CGM data alone to justify programming changes. Cross-reference with performance data and client self-report. |
| 3. Pattern Identification | End of month 1 | Look for three signals: pre-session glucose that correlates with poor session performance, post-session drops that correlate with reported fatigue, and overnight recovery pattern quality. | Do not present findings as medical conclusions. Frame as coaching observations: “Your data suggests your energy is most available in this window.” |
| 4. Programming Adjustment | Start of month 2 | Use pattern data to make one specific programming decision: session timing, pre-session nutrition window, or intensity sequencing across the week. Document the decision and the rationale. | Do not make more than one variable change at a time. CGM data cannot isolate causation. Change one thing, observe for two weeks, then adjust. |
The one-variable-at-a-time rule in step four deserves emphasis because it is where the workflow is most likely to break down. Clients who are engaged with their CGM data are often highly motivated, and motivated clients want to change multiple things at once. Resist that. If you adjust session timing and pre-session nutrition and training intensity in the same week, and the trace changes, you will not know what caused the change. You will have a better-looking trace and no useful information about why. Change one thing. Watch it for two weeks. Then decide what to do next.
The client who arrived with two weeks of annotated trace data eventually became one of the more interesting programming cases I have worked with. Not because the CGM revealed something dramatic. Because it gave both of us a shared reference point for conversations that had always been slightly vague before. “I feel better when I train in the morning” became something we could look at together rather than just take on faith. The data did not tell us why. It confirmed that the pattern was real and consistent, which was enough to make a programming decision with some confidence behind it.
That is the appropriate use of CGM data in a coaching context. Not a diagnostic lens. Not a replacement for clinical care. A shared reference point that makes the coaching conversation more specific. Coaches who treat it as anything more than that are likely to create more confusion than clarity. Coaches who dismiss it entirely are leaving a useful tool on the table. The line between those two positions is exactly where the scope-of-practice boundary lives.
Related: Coaching on GLP-1s: What Every Trainer Needs to Know Right Now
Coaches who can work fluently with client wearable data are exactly what performance-minded and tech-forward studios are hiring for. FitHire by Coach360 lists roles at studios building around data-literate coaching.
Can a fitness coach use CGM data to guide a client’s training program?
Yes, with a specific and important qualification. A coach can use CGM data to observe patterns in how a client’s glucose responds to training, sleep, and food timing, and can use those patterns to make programming decisions like session timing, intensity sequencing, or pre-session nutrition windows. What a coach cannot do is interpret specific glucose values as diagnostic indicators, suggest targets or ranges, or use the data to recommend changes to medication, supplementation, or clinical dietary interventions. The line is between pattern observation and clinical interpretation. “Your trace suggests your energy is most available in the late morning based on these two weeks” is a coaching observation. “Your fasting glucose is trending high and you should look into berberine” is not. That second sentence belongs with a physician or registered dietitian, not a fitness coach.
What does a normal glucose trace look like during a high-intensity training session?
During high-intensity intervals, it is common to see a glucose spike as the body releases stored glucose through glycogenolysis to meet the sudden increase in energy demand. In well-trained, metabolically healthy individuals, this spike can be significant and is not inherently a problem. Research in exercise physiology has documented that the glucose excursions seen in fit, non-insulin-resistant people during intense exercise can exceed the reference ranges displayed on consumer CGM platforms, and that those excursions resolve quickly and do not carry the same clinical significance they would in a person with metabolic disease. The practical takeaway for coaches: a spike during sprint intervals is not a red flag. A spike that does not resolve within 30 to 60 minutes post-session, paired with the client feeling unwell, is worth flagging to the supervising physician. Context matters more than the number.
Should I recommend that my clients try a CGM?
This sits at the edge of coaching scope and requires care. Recommending a specific health monitoring device to a client is adjacent to clinical advice, particularly for clients who have any history of metabolic concerns, are on medications that affect glucose, or who are already in a supervised program. A reasonable position is to be responsive rather than proactive: if a client asks about CGM directly, you can describe how the data has been useful in coaching contexts and suggest they discuss it with their physician before starting. What coaching scope does not cover is initiating the recommendation, suggesting a specific brand or sensor, or framing it in terms of health outcomes that belong in a clinical conversation. The distinction matters because clients hear recommendations from their coaches with a different weight than coaches sometimes intend. Being precise about where your expertise starts and ends is not a limitation on your effectiveness. It is what makes you someone a client can trust with information that actually matters.
How long does a client need to wear a CGM before the data is useful for training decisions?
The minimum useful period is about two weeks of training-day overlays, meaning two weeks of CGM data that includes session start times, duration, and subjective energy ratings logged alongside the trace. Less than that and you are looking at individual data points rather than patterns, and individual data points in CGM data are easy to misread. A single low reading before a session could be timing, sleep, stress, or nothing. Two weeks of consistent low pre-session readings that correlate with poor session energy is a pattern worth acting on. The practical workflow is to collect a baseline week of CGM data with no programming changes, then overlay two weeks of training-day data, then look for three specific signals: pre-session glucose that correlates with session quality, post-session drops that correlate with reported fatigue, and overnight recovery pattern. That three-signal read gives you enough to make one specific, testable programming adjustment, which is the appropriate scale of intervention for coaching-level glucose data.
This article is for educational purposes for fitness coaching professionals and does not constitute medical advice. CGM data interpretation for clinical purposes, and any decisions about medication, supplementation, or dietary intervention, belong with a physician or registered dietitian.
About Erin Nitschke
Dr. Erin Nitschke, NSCA-CPT, NFPT-CPT, ACE Health Coach, ACE-CPT, Fitness Nutrition Specialist, Therapeutic Exercise Specialist, Pn1, FNMS, and DSWI Master Health Coach, is a seasoned college professor in health and human performance. She is a nationally recognized presenter, industry writer for IDEA, NFPT, Fitness Education Online, and Youate.com, and an active member of the ACE Scientific Advisory Panel. With extensive experience in health and exercise science, Erin specializes in holistic, evidence-based approaches to wellness. Her passion lies in empowering individuals to lead healthier, more vibrant lives through personalized coaching. Erin’s philosophy centers on education, accountability, and sustainable behavior change—guiding clients to achieve long-term success in nutrition, fitness, stress management, and overall well-being. To connect with Dr. Nitschke, email her at erinmd03@gmail.com or on Instagram: @nitschkeerin
She came in on a Tuesday carrying a coffee she hadn’t touched. Eight months into training. A few weeks earlier, she had PR’d her deadlift. I looked at her Whoop band before we began and saw a recovery score of 31, resting heart rate up fourteen beats from her average, and HRV trending down. I swapped her session before she set her bag down.
That swap took forty seconds. The client did not feel like she was getting less out of her session. She felt like I was paying attention to how she was showing up. I kept that client for another two years.
That is what wearable data in coaching actually does when it is built into the system. Not the data itself, but the workflow that turns the data into a decision before the client walks through the door.
If you run a facility or manage a team of coaches, you have probably watched this play out on the wrong side. A coach with a stack of wearable screenshots from clients and no idea what to do with them. The data is there. A logical, thoughtful protocol is not.
The coaches who are retaining clients at high rates right now are not necessarily the ones with the best programming instincts. They are the ones who have built a repeatable intake and session-adjustment process around the data their clients are already generating. The difference is infrastructure and strategy.
Gyms sometimes treat wearables as a value-add: something to mention during the sales process and then hand off to the client to figure out. That is not integration. That is decoration. The gap is not data access. Your clients already have it. The gap is the layer between the data and the coaching decision.
Heart rate variability for coaches is not a reading to admire. It is an input that should change what happens in the next session. When HRV drops below a client’s personal average for three consecutive mornings, that is not an abstract warning. It is a concrete signal that the nervous system has not recovered, and if you push a high-intensity session on top of it, you are training into a hole. Some clients will white-knuckle through it and say nothing. Some will drop off.
The tradeoff is real and worth naming directly: using wearable data well requires your coaches to make calls that the client may not understand in the moment. Pulling back a session when someone feels ready to go is counterintuitive. You need a client education layer built into the process, or the data-driven adjustment reads as the coach being overly cautious.
This is not a fifteen-minute analysis. Coaches who do this well are spending two to three minutes per client, per day, on three specific numbers: HRV relative to personal baseline, resting heart rate trend over the prior five days, and sleep quality score. Not absolute values. They are looking for trends relative to the individual.
Personal baseline matters more than population averages. A resting heart rate of 58 means something completely different for a 42-year-old recreational lifter than for a former collegiate rower. Coaching with wearable technology is only useful when the reference point is the client in front of you, not a chart from the device manufacturer.
The three-point protocol produces one of three session calls: proceed as programmed, modify load and intensity by 15 to 20 percent, or pivot to active recovery entirely. For clients who push back on a modified session, the cue that tends to land is some version of: “Your body already trained hard last night. We’re here to support recovery.” That language reframes the modification as an extension of the work, not a reduction of it.
How to use Whoop data with clients starts before the first session. During onboarding, or during a quarterly check-in for existing clients, run a fifteen-minute data review. Not to interpret everything, but to establish the client’s personal baselines across four weeks and to set the thresholds that will trigger session modifications.
For Whoop users specifically, the strain and recovery pairing is immediately actionable for programming adjustments. A client coming in with a day strain already at 14 by noon, from a commute and two stress calls, is a different training input than the same client on a calm Sunday morning. Neither the client nor the coach is managing the numbers. They are managing the decision the numbers point to.
The intake structure runs four steps. First, connect the Whoop account or have the client screenshot that morning’s recovery report. Second, compare to the four-week rolling baseline established at onboarding. Third, apply the three-tier session call from the pre-session protocol. Fourth, note the call in the session log so patterns surface over time. A client who routinely shows suppressed HRV on Mondays is telling you something about their weekend that the programming should account for.
Owner-operators running multi-coach facilities: this is where coaching with wearable technology either scales or collapses. If each coach is using their own method of reading the data, the outcomes vary and the process cannot be replicated. A shared intake document, even a simple one built in Google Sheets, with the four-step structure means any coach can pick up any client and apply the same protocol.
Wearable data scope of practice is a liability concern that becomes real the moment a coach interprets a low HRV reading as a cardiac symptom or tells a client to see a cardiologist based on a consumer device. That is outside the lane.
The boundary is this: coaches use the data to make training decisions. Not diagnostic decisions, and certainly not medical referrals based on device readings. The three-tier session call (proceed, modify, or pivot) stays entirely within training programming. The moment the interpretation moves toward health status rather than readiness for physical effort, the coach refers to the appropriate provider or clinician and documents that referral.
Build that boundary into the coach training and into the client-facing materials. Clients who understand the difference between “your device is telling us your recovery is low, so we’re adjusting today’s session” and “your device is flagging a health concern” are less likely to conflate the two. It also raises the perceived professionalism of the process considerably.

Integrating wearables into training programs is not a retention strategy by itself. It becomes one when the workflow produces something clients can feel: the sense that coaching is adapting to them specifically, not running a template with their name at the top.
The operators who have built this into their systems report two consistent outcomes. First, clients who feel seen at the data level tend to communicate more. They check in when travel disrupts sleep. They flag stressful weeks before they show up undertrained and frustrated. The data creates an opening for a different kind of conversation. Second, the modification calls (the ones where a coach pulls back a session based on HRV) become retention moments rather than disappointments when the client understands why they are happening.
A facility running twelve coaches and three hundred active clients can track session modification rates by coach and correlate them to renewal rates. That is not a sophisticated analytics build. That is a column in a spreadsheet updated weekly. The coaches whose modification rate is zero are probably not reading the data. The coaches whose modification rate is 40 percent probably overcorrected. The ones in the 12 to 18 percent range, adjusting one in six to eight sessions based on wearable inputs, tend to show the highest retention. That is a number worth knowing.
Max Darsonval, founder of Velocity AI, frames the underlying problem with the current generation of wearables this way:
“The wearable category has gotten very good at telling you what already happened. Heart rate, sleep scores, recovery, it’s all rear-view. The problem is the training session ends before the data is useful.”
— Max Darsonval, Founder, Velocity AI
Darsonval continues:
“Velocity’s bet is that the value isn’t in the dashboard the next morning. It’s in the rep you’re about to do.”
— Max Darsonval, Founder, Velocity AI
That distinction matters for operators evaluating where the category is going. The first generation of wearable integration is morning-recovery data driving today’s session call. The next generation is in-session data driving the next rep. The operators building the workflow now are positioning their coaches to absorb the next wave without rebuilding the system.
FITHIRE — FIND CERTIFIED COACHES WHO TRAIN WITH DATA
The coaches who implement this workflow are not self-taught guessers. They understand wearable data in coaching at a protocol level and they know how to apply it without stepping outside their scope. If you are hiring for your facility or expanding your team, FitHire surfaces candidates with documented experience integrating wearable technology into client programming.
How do I use wearable data in coaching without overcomplicating my programming?
Start with one metric and one decision rule. Heart rate variability relative to personal baseline is the most reliable single input for session readiness. Set a threshold (say, HRV 15 percent or more below the client’s four-week average) that triggers a session modification. Apply that rule consistently for sixty days before adding additional data points. The complexity that kills most wearable integrations comes from coaches trying to build a dashboard before they have built a habit. One metric, one rule, one documented outcome per session. That is the foundation.
What is heart rate variability for coaches, and how is it different from resting heart rate?
Resting heart rate gives you a snapshot of cardiovascular load at a single moment. HRV gives you a picture of how well the autonomic nervous system is recovering between stressors: training, sleep disruption, psychological stress, illness. A client’s resting heart rate might look normal the morning after a hard block, but their HRV will often tell a different story. For coaching purposes, HRV is the earlier signal. It tends to drop before fatigue shows up as performance decline, which means a coach with HRV data can make a training adjustment before the client hits the wall rather than after. Most consumer devices (Whoop, Oura, and Garmin) measure it during sleep and provide a morning readiness score based on HRV trends.
What are the scope of practice rules for coaches using wearable data with clients?
Coaches use wearable data to make training decisions: whether to proceed with a planned session, reduce load, or shift to recovery work. That is the full scope. Interpreting a device reading as a symptom, recommending medical follow-up based on device outputs, or making health claims based on wearable data falls outside coaching scope regardless of the device’s accuracy. Some clients will ask their coaches to weigh in on what a low HRV reading means for their health. The correct response is that you are using the number to inform today’s training, not to assess their cardiovascular health, and that questions about health should go to their physician. Document the referral. This distinction also matters for liability: a training adjustment based on a recovery score is a coaching call. A diagnostic claim based on a recovery score is not.
How do I build wearable data into a multi-coach facility without the process falling apart?
The single-document problem is where most multi-coach facilities stall. If the intake protocol lives in each coach’s head, it does not scale and it does not transfer. Build a one-page shared intake template with three fields: today’s recovery data, comparison to the client’s rolling baseline, and today’s session call (proceed, modify, or pivot). Every coach fills it out the same way. Review the calls weekly in your team meeting. Over sixty to ninety days you will see which coaches are actually using the data and which are skipping the check. The aggregate data also tells you things at the facility level: if modification calls spike every Monday across the board, your weekend programming is probably pushing too hard. That is a facility-level insight you only get when the data is standardized across coaches.
Erin Nitschke is a Coach360 contributing editor covering coaching technology, wearable integration, and the operational systems behind high-retention training businesses.
About Erin Nitschke
Dr. Erin Nitschke, NSCA-CPT, NFPT-CPT, ACE Health Coach, ACE-CPT, Fitness Nutrition Specialist, Therapeutic Exercise Specialist, Pn1, FNMS, and DSWI Master Health Coach, is a seasoned college professor in health and human performance. She is a nationally recognized presenter, industry writer for IDEA, NFPT, Fitness Education Online, and Youate.com, and an active member of the ACE Scientific Advisory Panel. With extensive experience in health and exercise science, Erin specializes in holistic, evidence-based approaches to wellness. Her passion lies in empowering individuals to lead healthier, more vibrant lives through personalized coaching. Erin’s philosophy centers on education, accountability, and sustainable behavior change—guiding clients to achieve long-term success in nutrition, fitness, stress management, and overall well-being. To connect with Dr. Nitschke, email her at erinmd03@gmail.com or on Instagram: @nitschkeerin
A client walks in for session three with clean nutrition, full attendance, and every rep counted. Midway through the warm-up, the energy is gone. Your push cues are not landing. Yet nothing seems wrong on the surface. Understanding mental wellness — where this client sits on the dual-continuum — is the first step, not the last.
Traditionally, mental health framing uses a single axis, ranging from severe illness to no illness. By adding a vertical dimension, the model captures what the single axis misses. At the top sits flourishing: clients who thrive, set PRs, and drive their own sessions forward. Languishing sits at the bottom. Yet these clients have no clinical diagnosis. They feel stuck, flat, and cut off from progress.
Mental wellness in this framework is not the absence of illness. It is an active state. A client can be entirely free of any clinical diagnosis and still operate in a languishing state. Pushing hard on that client does not produce a breakthrough. Instead, it often speeds up dropout, injury, or burnout.
This model does not ask coaches to become therapists. Instead, it asks coaches to notice which quadrant a client occupies and respond. The honest limit worth naming: this is an orientation tool, not a clinical one. It sharpens your read of the room. It does not replace assessment by a licensed mental health provider.
Sharon Gam, PhD, trains clients in strength work and mental wellness. Before each session, clients rate their mood, energy, stress, and self-confidence on a 1–10 scale via a short Google Form. They write a workout intention on a whiteboard during warm-up. This is not a long-term goal. Instead, it is something specific they want to feel or achieve that day.
“Depending on what they write, I might ask why that intention matters today,” Gam says. “It opens a talk that points me toward their mental wellness.” Third comes the session close. She asks clients to reflect on what they set out to feel versus what they felt. That step helps clients notice progress they would otherwise miss.
Here are four intake questions coaches can embed in a standard check-in:
The answers will not produce a clinical picture. They will tell you whether to reduce load, restructure the session, or check in next week. Gam documents responses in session notes and tracks patterns. Clients who score low in heavy work periods show a mental wellness signal she would not otherwise catch.
“Often I notice recurring patterns. These help me shape the long-term program and open talks about their mental wellness over time.”
SHARON GAM, PHD. PERSONAL TRAINER. STRENGTH AND MENTAL WELLNESS
The dual-continuum model draws the boundary as clearly as it defines the framework. You adapt sessions, add breathing cues, and run check-ins. You do not diagnose or treat. When check-ins show repeated low scores or outside disruption, your role changes. It shifts from modifier to navigator.
Gam builds her referral network with care. “The right fit matters with mental health providers, just as it does with fitness providers,” she says. “I meet providers in person before I recommend them. If I know them, I can describe their style to a client. That makes the referral land.” Keep a short list of two or three mental health providers whose work you know.
The language that works sounds like this: “You have been consistent in training. Some patterns suggest added support could help. I would like to connect you with a mental health provider.” Frame it as a skilled recommendation, not a critique. That framing keeps the relationship intact and gets the client to act.
Detecting languishing does not mean removing challenge. Instead, it means aligning the session to what the client can absorb that day. When intake signals languishing, use three moves. First, reduce circuit length and add variety to cut cognitive load. Second, build in one brief social exchange between sets. Third, add a single directed breath cue during rest. Not a full block. Just a 10-second focus reset between compound movements.
For clients showing signs of flourishing, maintain intensity. Use their strong mental state to push for a PR or test new movements. Weekly check-ins tracked alongside training metrics reveal patterns worth acting on. A client who languishes in busy work weeks but recovers after social events shows a mental wellness signal. You would not find it in load data alone.
The honest tradeoff: check-ins add two to three minutes per session. Added late in the coaching relationship, they can feel out of place. Added from day one as part of intake, clients treat them like any other standard step. According to the Global Wellness Institute, adding wellness to exercise programs shows gains in both reducing illness and building flourishing states.
“Focusing on mental wellness has been good for my business,” Gam says. “I attract my ideal clients, my clients stay longer, and my clients are happier.” She states this clearly on her website. Mental wellness is how she stands apart in fitness. That is not a branding result. It is a systems result.
Studios that run mental wellness check-ins protect clients and grow staff skill. Coaches who read the dual-continuum model respond to what is happening rather than guessing. Lower coach burnout is a real lever. It starts with intake that gives coaches a frame for what they see on the floor.
Record your check-in process in writing. It signals rigor and protects your scope of practice. When built into onboarding, it creates a training floor for any coach you hire or manage. Studio owners who add this to onboarding build a culture where mental wellness signals get the same care as training data. That consistency turns a reactive team into one that drives retention.
FOR COACHES READY TO APPLY
Coaches who build mental wellness into their practice can find aligned studios on FitHire by Coach360. Create your profile and let your method speak for itself.
How often should I run these mental wellness intake questions?
First, run a full check-in at initial intake. From there, a two-question version at the start of each session takes under two minutes. Subtle shifts in energy and focus are almost always the first sign that a client is drifting toward languishing.
What if a client resists mental wellness talks?
Instead, frame questions around performance: energy levels, sleep quality, training focus. Most clients who resist mood-based framing engage with output framing right away. You get the same data under a different label.
How do I initiate a referral without damaging the coaching relationship?
Use language tied to what you have seen: “You have been consistent. I want to make sure you get full support. I would like to connect you with someone in this area.” Frame it as adding support, not ending your work together.
Can the dual-continuum model work in group fitness?
Yes. In group settings, read the room rather than asking direct questions. Observe energy, focus, and presence. Adjust pacing, offer brief rest intervals, or add a mindful transition. Address visible languishing signals across the group without singling anyone out.
Bloodwork for coaches has long been useful in theory and hard to act on in practice. When a client does everything right — three sessions a week, meals tracked, sleep improving — the pattern should show results. Yet four months in, recovery still lags. Check-ins don’t explain it. The usual levers have been adjusted. Still, the client is stuck.
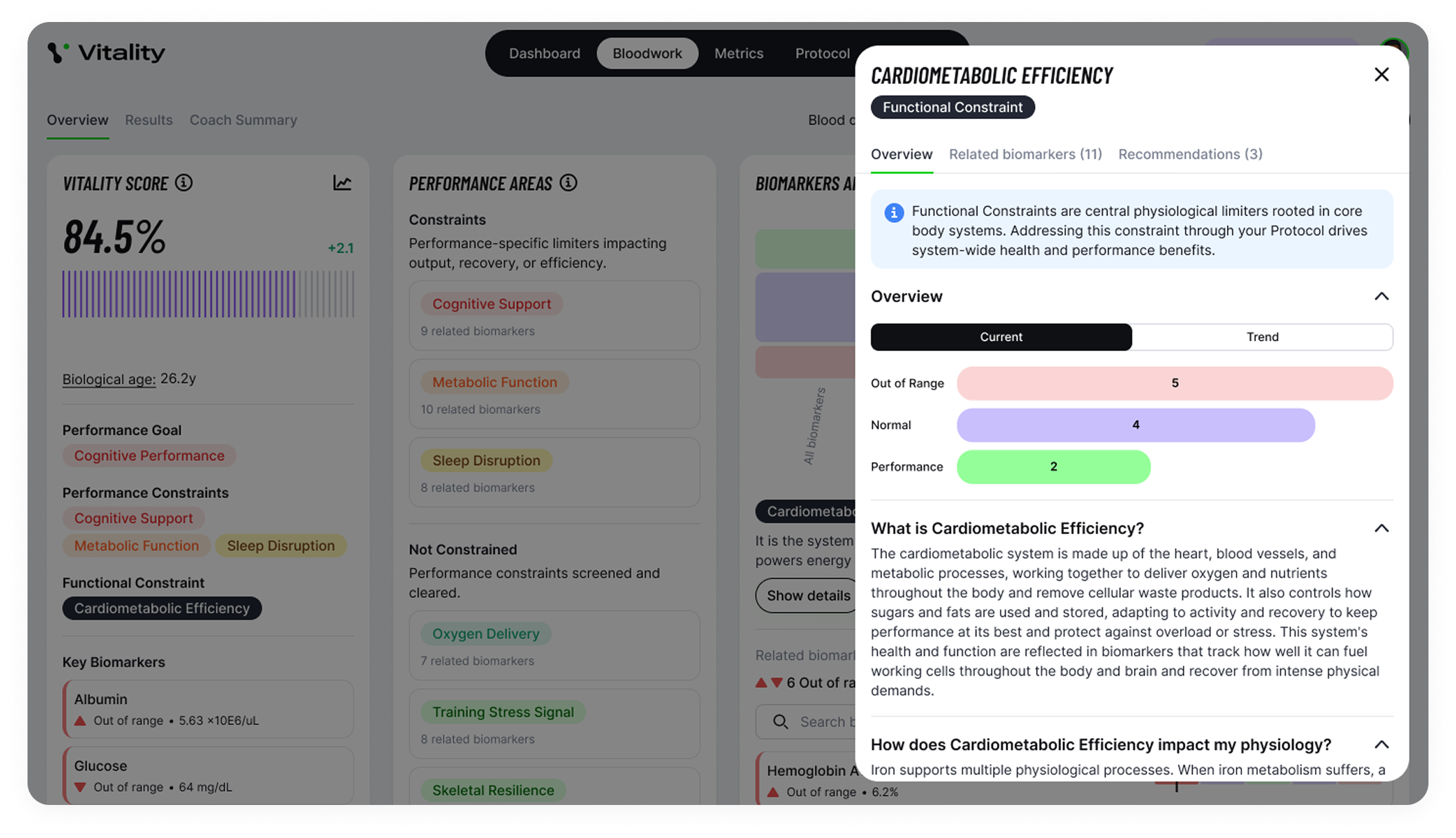
For coaches, the barrier was never interest. Most could see the value in lab data. But the reading was the wall. Reading biomarkers and explaining what they mean sits close to a legal line. Yet coaches have no reason to cross it. Vitality Blueprint was built around that specific problem. For coaches worried about scope, the platform draws the line. It does not ask them to read labs. Instead, it reads them, runs the analysis, and gives coaches a protocol to deliver. That takes the legal and ethical risk off the table.
At the center of the platform is the Key Constraint model. The system runs more than 20,000 data runs across 100-plus biomarkers. After that, it scores 13 functional areas. Then it identifies the single biggest bottleneck holding the client back. For a coach whose client is tired and can’t recover, that framing changes the session. The issue may not be effort or discipline. It could be subclinical iron depletion, a poor cortisol-to-DHEA ratio, or a vitamin D level that reads normal but falls short for hard training.
Standard reference ranges are built from broad populations. Being in range can still leave a client flat, under-recovered, and stalled. Instead, Vitality targets performance markers, not disease ranges. That gap is what bloodwork for coaches is designed to close. For most clients, the questions are direct: why do they gas out by 3 PM, why did gains stop, and why isn’t rest producing the recovery their effort should earn.
Dan Garner and Dr. Andy Galpin built this from environments where a wrong call showed up fast. Garner spent 15 years reading labs in combat sports and pro teams — fields where small errors carry visible performance costs. Galpin runs the Center for Sport Performance at Cal State Fullerton and has worked with NBA, MLB, and Olympic athletes. Neither built this from wellness language. They built it from cases where the bloodwork explained what the training data couldn’t.
For both, the argument is that elite and general physiology are not separate systems. Iron still carries oxygen. Cortisol still shapes sleep. Thyroid, testosterone, inflammation, and gut function still affect energy and recovery — whether the client is preparing for a world title or just trying to stop fading by 3 PM. But what changes is context. An NBA player may be hunting the last two to five percent. A 42-year-old who trains three days a week and fades by 3 PM has bigger, more obvious gaps. For that client, a core protocol produces more visible results in a single 13-week cycle.
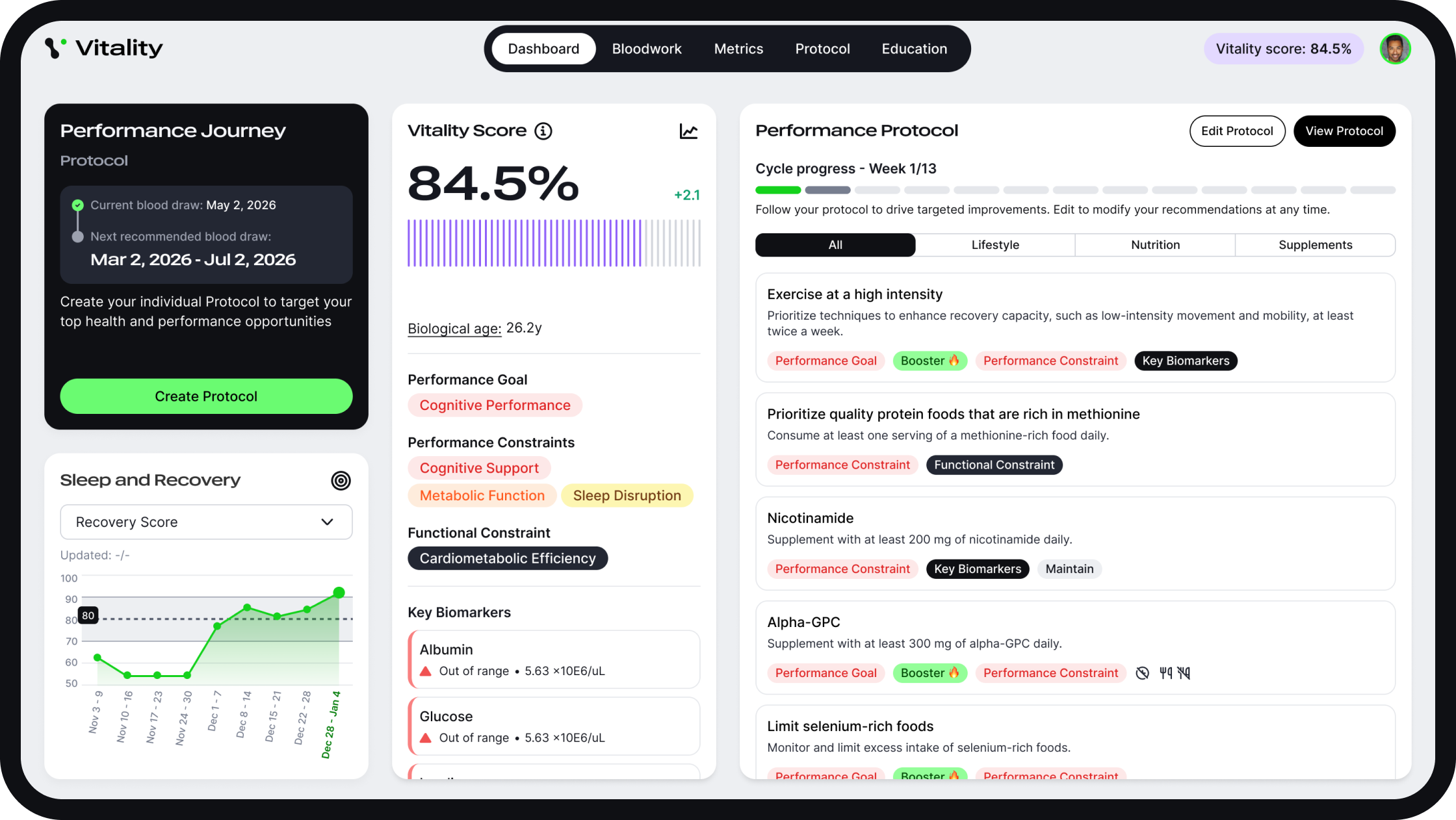
The workflow is clean. A coach signs up. The client gets bloodwork drawn at a standard lab. After that, results get uploaded. Analysis returns within seconds. Then the system finds the Key Constraint and builds a 13-week protocol. The coach delivers it. Without the platform, the coach is guessing at the explanation. When using it, they coach around a defined bottleneck.
“Instead of guessing, you coach around a defined bottleneck. The issue may not be effort. It could be subclinical iron depletion or a cortisol ratio that’s been off for months.”
DAN GARNER. CO-FOUNDER. VITALITY BLUEPRINT
Coaches can bundle Vitality into a premium tier or offer it as an add-on. In practice, the value conversation shifts. A client is no longer paying for reps, check-ins, or macros. Instead, they pay for a test, a plan, a 13-week cycle, and a retest. That structure gives clients clearer markers to track. It also gives coaches a natural retention system. When the 90-day retest is framed from day one, it does not feel like a late upsell. It feels like part of the process, because it is.
When clients understand what is limiting them and see that constraint shift 13 weeks later, they stay. When they stay, the proof is personal and measurable. That is harder to replicate in a standard model where progress fades after the first obvious gains. It works because it makes the cause visible before the fix is delivered.
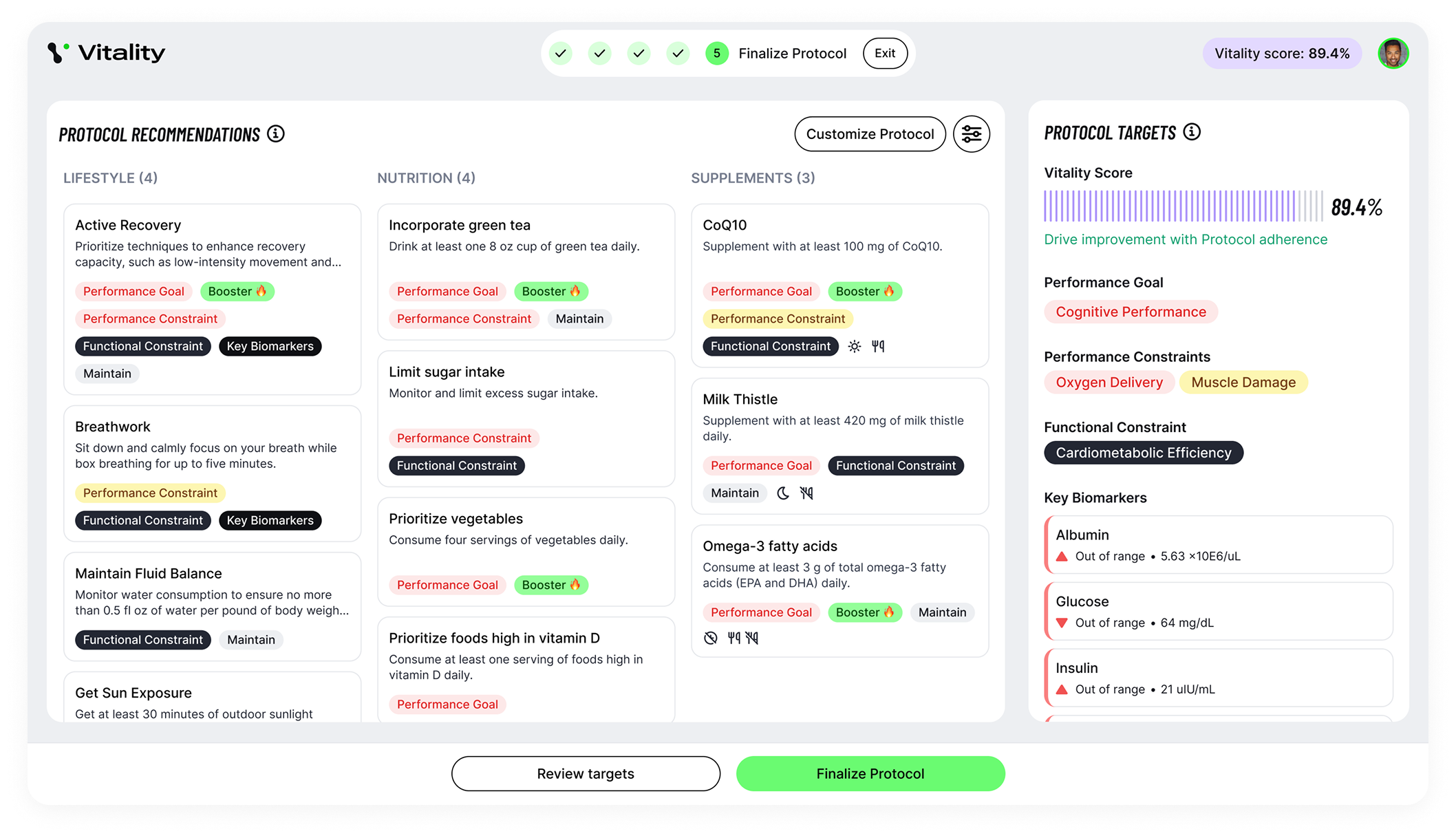
By design, the platform draws the scope boundary. Coaches do not diagnose or treat. Instead, they adapt sessions and adjust load based on what the Key Constraint shows. The system gives coaches one priority constraint and a plan, not a clinical picture. That keeps the work inside coaching. Vitality’s position is straightforward. Performance metrics — muscle mass, aerobic capacity, strength, and energy output — are better daily health guides than a fear of disease. Coaches don’t need to compete with peptide clinics or prescription-driven centers. They stay in performance, recovery, and behavior change — and the bloodwork drives the conversation without a medical credential.
Still, early reviews include coaches and practitioners with strong standing: Tim Jones from Precision Nutrition, Megan Young from the Seattle Sounders, Jill Miller from Tune Up Fitness, and Adam Dupas from Combat Fitness. But the stronger case is simpler. When clients see their own data, they understand the likely cause of their fatigue or stalled recovery. Then they return 13 weeks later with a measurable result. That is the proof point that builds the practice.
Studios adding bloodwork for coaches as a service need practitioners who can connect health data with training and recovery without drifting outside their scope. That is a hiring problem before it is a service problem. Adding it only holds if the coaches on the floor can handle the conversation. For operators building this capability, the selection challenge comes first.
For coaches, the instinct was always there. For most of their careers, they just couldn’t act on it safely. Now they can.
FOR OPERATORS BUILDING THIS CAPABILITY
Find coaches built for data-guided work on FitHire by Coach360. Post your role today.
Does using Vitality Blueprint require a medical or nutrition license?
No. The platform keeps coaches inside their scope. Instead of reading raw lab data, the coach delivers a 13-week protocol based on the system’s output. The boundary between coaching and medicine stays intact by design. Coaches do not make clinical calls. They follow a structured plan built from the analysis.
How does adding bloodwork for coaches change client pricing?
The model shifts the value conversation. Instead of selling reps or check-ins, coaches offer a test, a 13-week plan, and a 90-day retest. That cycle gives clients clear markers and gives coaches a reason to stay engaged past the first phase. Most coaches add it as a premium tier or standalone add-on, priced above their base service.
What kind of bloodwork does a client need?
Clients get bloodwork at a standard lab — the same type used in a routine physical. No specialty clinic is needed. Results get uploaded to the platform and run against more than 100 biomarkers across 13 functional areas. The process works with what most clients can access, not a boutique health panel.
Is Vitality Blueprint built for personal trainers or clinical practitioners?
Personal trainers and performance coaches are the primary users. The platform was designed to make lab data useful without a clinical background. Dan Garner and Dr. Andy Galpin built it from elite performance work, but the model applies across client types. The biomarkers stay the same whether the client is an Olympic athlete or a 42-year-old who trains three days a week.
About Robert James Rivera
Robert is a full-time freelance writer and editor specializing in the health niche and its ever-expanding sub-niches. As a food and nutrition scientist, he knows where to find the resources necessary to verify health claims.

![]()
Powering the Business of Health, Fitness, and Wellness Coaching