All Categories
All Categories
Clinical data fitness coaching clicked for me when I watched a client stop arguing with the plan the moment the data made the problem visible. For weeks, she thought the issue was effort. Her scan showed lean mass had dropped. Her waist had barely moved, and her strength numbers had stalled.
The numbers worked because they told us what to change next, not because they sat in a report nobody used.
If you coach real clients, you already know the obvious version. Intake form, body comp scan, progress photos. Maybe a wearable dashboard. The gap is what happens after that first readout. Data only becomes revenue when it changes the next block, triggers a scheduled reassessment, and gives the client a clear reason to keep going.
A body composition scan, movement screen, wearable trend, blood pressure reading, or recovery score has value only when it changes the plan. This is where clinical data fitness coaching becomes useful: the coach turns the number into the next programming decision.
Research on personal health data in coaching points in the same direction. Personal health data gives coaches more objective insight into client behavior, but its value depends on how well it shapes the next coaching decision.
The client trusts you to show what the report means, what has to change, and when you’ll check it again. Use this coaching cue in the review to move the client from vague hope to a clear next step:
“We’re not guessing for six more weeks. This number tells us what the next block has to solve.”
Use a simple framework. Call it the 6-week reassessment cycle. A useful reassessment framework for fitness coaches connects every metric to a decision, not a dashboard.
The loop has five parts:
That gives you a clean 6-week reassessment cycle without adding busywork. Six weeks gives the training block enough time to show movement in strength, body composition, nutrition follow-through, or recovery trends. It also keeps the client close to the next decision instead of drifting through another vague month of workouts.
Example:
A client starts with baseline data:
You build the next 6 weeks around the metric that matters most. Then you reassess and show the client what changed.
ACSM’s fitness assessment manual organizes testing across body composition, cardiorespiratory fitness, muscular fitness, and flexibility. That gives coaches a clear assessment lane, as long as the data gets tied to training decisions and referral boundaries.

Don’t track everything. Track the metrics that change what you prescribe.
A strong starting set for coach-driven health data is:
Body composition tells you whether weight change is moving in the right direction. InBody’s educational material frames body composition as more specific than scale weight. It breaks weight into components like fat mass, lean mass, water, protein, and minerals. It can also show change over time in fat mass, lean muscle mass, and body fat percentage.
Strength performance tells you whether the training signal is holding. If scale weight drops and load drops every week too, you have a problem. If fat mass drops while strength stays steady, the plan has more room.
Resting heart rate or recovery trend gives you a simple fatigue flag. It isn’t a diagnosis. It is a programming signal.
This is where premium coaching services become easier to sell. The client sees the rule before the result.
Use hard triggers. The coach who can say, “This is the trigger, this is the adjustment, and this is when we retest,” has a stronger offer than the coach selling another month of workouts.
| Trigger | Coaching Decision |
|---|---|
| Body fat does not move after 6 weeks and adherence is above 80% | Change the nutrition process or raise activity targets |
| Lean mass drops more than 1% across the reassessment window | Reduce conditioning volume and increase protein priority |
| Resting heart rate is up for 7 days and session quality is down | Pull back intensity for 3 to 5 days and check sleep, stress, and intake |
| Grip strength drops across 2 straight checks | Reduce fatigue load before adding more work |
| Waist measurement is unchanged after 6 weeks while weight drops | Inspect hydration, food quality, and muscle loss risk before celebrating the scale |
| Strength on key lifts drops for 2 straight sessions | Hold load and reduce accessory volume |
| Blood pressure reads outside a safe exercise range | Stop intensity progression and refer the client to a licensed medical provider |
Use one repeatable lift as the performance marker. For example, track a trap-bar deadlift, goblet squat, or bench press for 3 working sets of 5 to 8 reps once per week.
Keep the test conditions consistent: same exercise, rep range, rest window, and point in the training week. Give the client 48 to 72 hours before repeating the pattern hard again, then progress load only when reps, form, and session quality hold.
At week 6, compare the lift, body composition, waist measurement, and recovery notes. If strength drops for 2 straight sessions, hold load and reduce accessory volume before adding more work.
The report is a moment. The reassessment cycle is the service.
A clean 6-week offer can include:
You’re not charging for a machine reading, but for interpretation inside your scope, programming changes, follow-up, and review. The data review belongs inside the paid cycle. It’s not meant to serve as a free explanation before the client decides whether to continue.
MedVanta fits this model because it connects clinical insight with the coaching decision that follows. For operators, that turns assessment data into a clearer service path, not a one-off report.
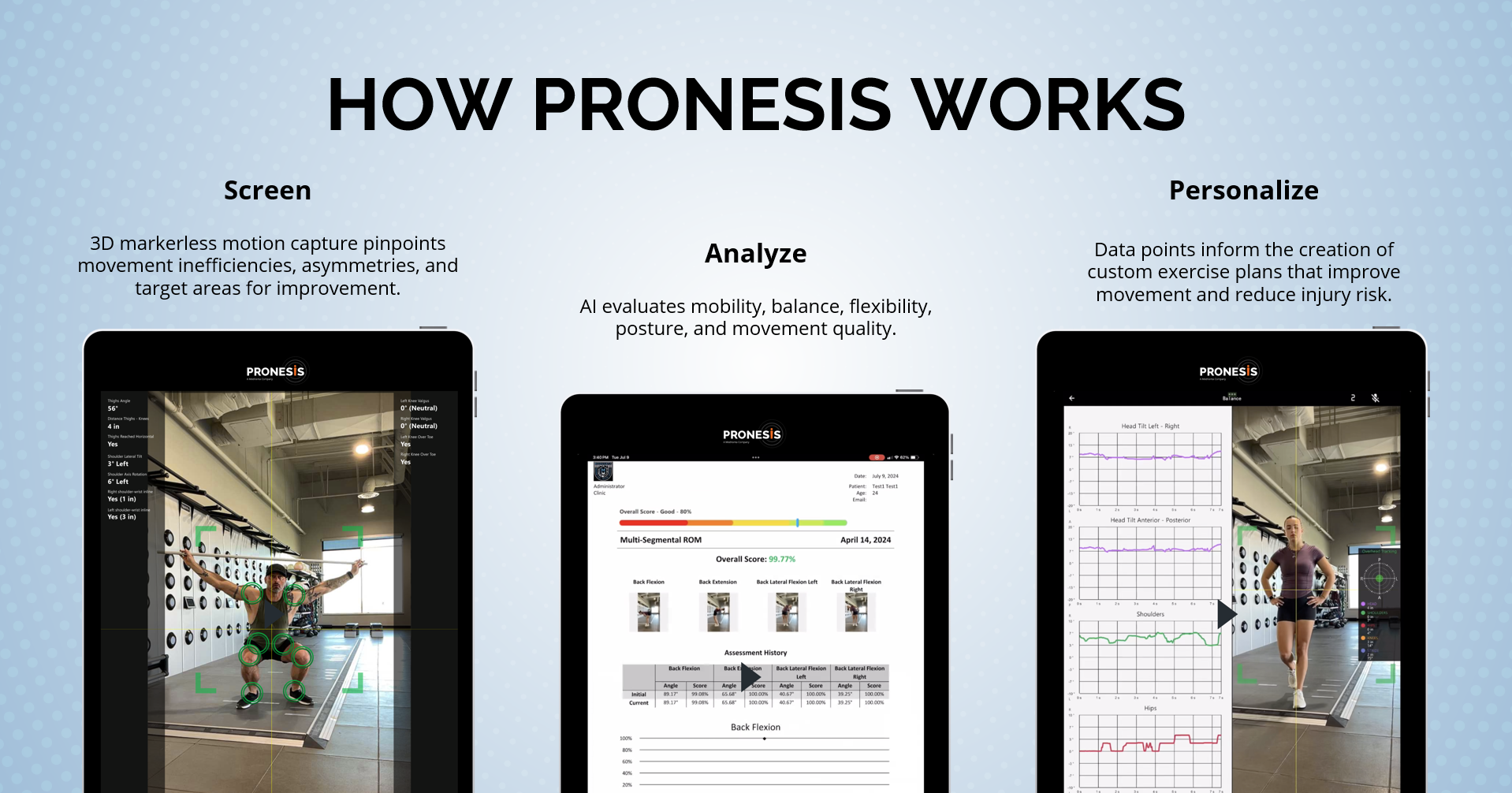
“Rather than completing generic assessments, that turn out variable and subjective results, Pronesis delivers clear and objective data showing the client’s dysfunction in their movement patterns, which can lead to decreased performance and possible musculoskeletal injury. This data shifts the conversation from ‘Do I need this?’ to ‘How do we fix this?'”
— Chuck Bollacker, MHA, PTA, Director of Business Development and Implementation, Pronesis, a MedVanta Company
Coaches don’t diagnose, prescribe medical treatment, interpret disease markers as medical findings, or tell clients to ignore clinician advice. Use clinical data to guide coaching decisions and refer when the data points outside training scope. This protects the client and the coach.
A high blood pressure screen belongs to a licensed medical provider. So do chest pain, unusual shortness of breath, fainting, unexplained symptoms, or lab results that look abnormal. You can adjust training around the information you are qualified to use, but medical interpretation stays with the ordering clinician.
You have to document better, run reviews on schedule, and explain data in plain language without drifting outside scope. You also have to train clients to care about more than the scale.
A 6-week reassessment cycle forces cleaner work. If the client knows you will retest in 6 weeks, the plan cannot stay vague. The training block needs a target, check-ins need a purpose, and the review needs a decision.
The review has one job: show the client what changed and what happens next.
Use this format. Here is what…
A client who sees progress has a reason to continue. Likewise, a client who sees the wrong metric move also has a reason to continue, if you can explain the correction. The data doesn’t close the sale by itself; the review does.
Body composition tools already show how training, nutrition, and lifestyle changes can become visible over time. InBody’s body composition analysis material describes tracking response to nutrition, physical activity, and lifestyle interventions as a way to turn data into actionable insight.
Coaches who can turn assessment data into clear training decisions are becoming more valuable in performance-driven settings. Browse roles at FitHire by Coach360 if you want to work where reassessment, strength planning, and coach-led systems carry real weight. www.fithirebycoach360.com.
What is clinical data fitness coaching?
Clinical data fitness coaching uses assessment data, such as body composition, performance markers, recovery trends, and referral-aware health screens, to guide training decisions. The coach uses the data to adjust programming and refer out when the issue sits outside training scope.
How often should a coach reassess clients?
Use a 6-week reassessment cycle for most coaching blocks. Six weeks gives enough time for a training change to show up, while keeping the client close to the next decision.
What data should a personal trainer track first?
Start with body composition, strength performance, and a simple recovery marker such as resting heart rate or session-quality trend. Add more data only when it changes a coaching decision.
About Robert James Rivera
Robert is a full-time freelance writer and editor specializing in the health niche and its ever-expanding sub-niches. As a food and nutrition scientist, he knows where to find the resources necessary to verify health claims.
Recovery services for gyms are moving from amenity to operating infrastructure — and the clubs that treat them as a business strategy rather than a wellness trend are the ones keeping members active, progressing, and renewing. MedVanta, a musculoskeletal health and prevention platform built for fitness operators, is making a specific case for why that shift is already happening and what it costs operators who wait.
Robert James Rivera spoke with MedVanta about the business case for recovery, the most common injuries operators are missing before they become retention problems, and how AI-powered movement screening is changing what is possible inside a fitness facility.
The demand signal is coming from members, not from operators. As strength training, recreational sports, and high-intensity workouts continue to grow, members are arriving with more movement limitations, overuse patterns, and recovery challenges than most gym programming was designed to handle. What they want has also changed — not just results in the next 12 weeks, but the ability to stay active and physically capable for the next 12 years.
Specifically, this shift is exposing a gap in how most clubs are structured. A facility built around performance output — sessions delivered, weights lifted, classes attended — is not the same facility as one built around sustained member capacity. The clubs noticing that gap are the ones starting to invest in recovery services for gyms as a core offering, not a premium add-on.
MedVanta frames the change in direct business terms: members who feel better, train longer, and trust the club’s expertise are more likely to remain loyal, engage with additional services, and maintain their membership for years. The inverse is equally direct. Members who hit an injury ceiling often do not come back.
“Members who feel better, train longer, and trust the club’s expertise are more likely to remain loyal, engage with additional services, and maintain their membership for years.”
— MedVanta
The musculoskeletal issues MedVanta sees most frequently in active adults are not dramatic acute injuries. They are predictable and gradual. Low back pain, knee pain, shoulder discomfort, tight hips and hamstrings — particularly among members who spend long hours sitting and then transition directly into high-intensity workouts without adequate preparation. The underlying pattern is consistent: mobility limitations, muscle imbalances, and repetitive movement patterns that gradually place stress on specific joints or muscles over time.
Importantly, none of these are inevitable. They are detectable before symptoms develop — if clubs have a mechanism to look for them. Simple movement assessments can reveal limited mobility, asymmetry, balance deficits, or poor stability that increase injury risk during exercise. When trainers have visibility into how a member moves, they can modify training and incorporate corrective exercises before a limitation becomes a disruption.
Furthermore, the catch for most facilities is structural: the member joins, completes a basic health form, and starts training without any baseline movement data on file. The club has already invested in a relationship before it has any insight into what that member is managing physically. By the time an injury surfaces, the disruption is already in progress.
MedVanta outlines a specific three-step sequence for clubs building a prevention culture without a facility renovation or a new staffing model.
First, incorporate a movement screening into new member onboarding. The screening establishes a movement baseline at the point of entry — before training begins, before limitations become problems, and before the club has invested in a relationship that gets interrupted by injury. A baseline gives trainers objective data. Without one, programming is based on self-report, which members consistently overestimate.
Second, provide coaches with tools and education to recognize mobility limitations and integrate corrective exercises into regular programming. This does not require a specialist hire. It requires giving existing coaches a framework for what they are seeing and a library of responses they can apply within sessions. The training investment is manageable. The retention impact is not.
Third, normalize recovery and movement quality as part of the training experience. Specifically, this means mobility work, proper warm-ups, and recovery strategies built into the culture of the facility — not positioned as something clients pursue independently. Members who see their coach treating recovery as a serious training variable are more likely to adopt that view themselves, and that behavioral shift compounds over time.
“The most effective approach is to embed recovery and prevention into processes that already exist within the club. Recovery strategies such as mobility work, corrective exercises, and education can then be layered into existing programming, so they enhance training rather than compete with it.”
— MedVanta
Movement and mobility assessments can serve as both a revenue-generating service and a high-value entry point for individualized programming. An assessment that gives a member a documented corrective plan justifies a session package upgrade and creates a record the member associates with the facility’s expertise.
Additionally, there is growing opportunity in trusted referral pathways for members who need clinical support beyond coaching scope. When a member develops persistent pain or a potential injury, clubs that guide them to qualified musculoskeletal providers quickly — without confusion — keep that member connected to the facility even during periods when they cannot train at full intensity. The alternative is a member who disappears for six to eight weeks, loses momentum, and cancels.
MedVanta’s Pronesis platform sits at this intersection. It is an AI-powered movement screening tool that analyzes how a person moves, identifies limitations and asymmetry in a few minutes, and gives trainers objective programming data. When a member needs clinical support, MedVanta connects them to trusted musculoskeletal care providers.
The honest tradeoff: implementing a recovery services model requires investment in staff education, screening infrastructure, and referral relationships before it generates revenue. Clubs that treat it as a quick revenue add-on without supporting systems see low uptake. The model works when recovery is embedded from onboarding — not offered as an optional upgrade six months into a standard membership.
Find Coaches With Recovery and Prevention Competency
FitHire by Coach360 connects clubs and studios with coaches who bring movement screening, corrective programming, and recovery-informed training to their sessions from day one.
MedVanta sees collaboration between fitness facilities and medical providers not as a future scenario but as an active transition. Fitness facilities are often the first place where movement limitations, pain, or injury risk can be identified — before a member visits a doctor, before a complaint becomes a diagnosis, and before an issue requires significant intervention. Clubs with trusted provider relationships can move members through that continuum without losing them.
Notably, this changes what the club represents in the member’s life. A facility that is only a place to exercise competes on equipment, price, and convenience. A facility that actively supports how members move, train, and stay active over time occupies a different category. “A partnership allows clubs to expand their role from a place where people work out to a place that actively supports how members move, train, and stay active long term,” MedVanta says.
Moreover, the five-year outlook MedVanta describes is an integration, not a revolution. Movement assessments, mobility work, and recovery strategies become routine parts of how members train and how coaches guide them. The clubs that begin building this infrastructure now — before it becomes standard — will be positioned to lead rather than follow. Those that do not risk falling behind as member expectations continue to evolve.
About Robert James Rivera
Robert is a full-time freelance writer and editor specializing in the health niche and its ever-expanding sub-niches. As a food and nutrition scientist, he knows where to find the resources necessary to verify health claims.

![]()
Powering the Business of Health, Fitness, and Wellness Coaching